











有什麼可以使子宮內膜瞬間變厚?反敗為勝,


子宮內膜變厚要用荷爾蒙,以及血管刺激因子的藥物。
這個是美國紐約方面的研究,至於如果妳要讓子宮內膜變厚,並不需
戲劇化增加試管嬰兒成功的~G-CSF
有什麼新的試管嬰兒技術?
你好:GCSF是針對子宮內膜薄,而試管嬰兒失敗的個案,請看以
GCSF目前在美國食品藥物管理局(FDA)是允許用在病人身上
戲劇化增加試管嬰兒成功的~G-CSF~
G - CSF的治療可改善IVF週期中子宮內膜不足
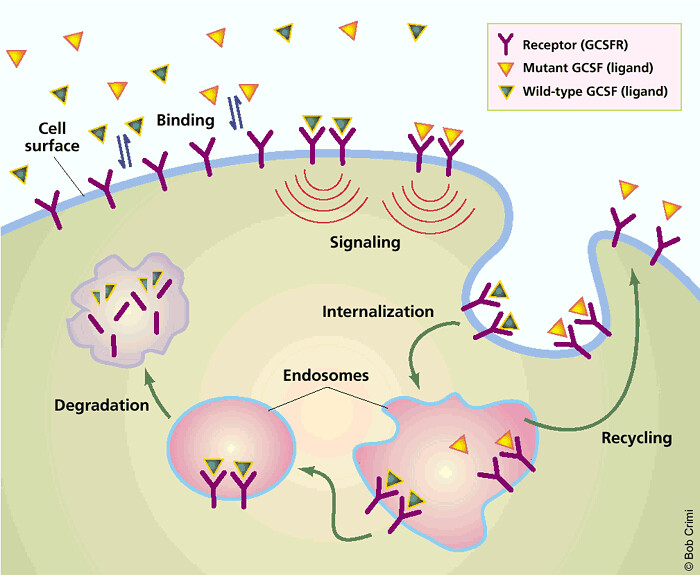
在體外授精(IVF)的週期,治療的藥物稱為粒細胞集落刺激因子
的G - CSF是一種細胞因子(蛋白質分子之間的溝通,以促進細胞)已被
研究人員從紐約市的中心人類生殖(CHR)的紐約州和生育第二個
在大約 1%的IVF週期,子宮內膜薄停留太成功植入胚胎,即使治療。在
“傳統的治療方法的不足,子宮內膜有參差不齊的成功最好的。無G - CSF的灌注,這些患者中,有可能,就不會達到胚胎移植,”解釋
“療效的G - CSF的改善子宮內膜,並有可能懷孕率在一般情況下,仍然需要在
博元婦產科不孕症試管嬰兒中心:蔡鋒博,陳昭雯醫師
原文:
A pilot cohort study of granulocyte colony-stimulating factor in the treatment of unresponsive thin endometrium resistant to standard therapies.
Abstract
STUDY QUESTION:
Is thin endometrium unresponsive to standard treatments expandable by intrauterine perfusion with granulocyte colony-stimulating factor (G-CSF)?
SUMMARY ANSWER:
This cohort study is supportive of the effectiveness of G-CSF in expanding chronically unresponsive endometria.
WHAT IS KNOWN ALREADY:
In a previous small case series, we reported the successful off-label use of G-CSF in four consecutive patients, who had previously failed to expand their endometria beyond 6.9 mm with the use of standard treatments.
STUDY DESIGN, SIZE AND DURATION:
In a prospective observational cohort pilot study over 18 months, we described 21 consecutive infertile women with endometria <7 mm on the day of hCG administration in their first IVF cycles at our center. All previous cycles using traditional treatments with estradiol, sildenafil citrate (Viagra™) and/or beta-blockers had been unsuccessful. G-CSF (Nupogen™) was administered per intrauterine catheter by slow infusion before noon on the day of hCG administration. If the endometrium had not reached at least a 7-mm within 48h, a second infusion was given following oocyte retrieval. Primary and secondary main outcomes were an increase in endometrial thickness and clinical pregnancy, respectively. Endometrial thickness was assessed by vaginal ultrasound at the most expanded area of the endometrial stripe.
PARTICIPANTS/MATERIALS, SETTINGS AND METHOD:
This study was uncontrolled, each patient serving as her own control in a prospective evaluation of endometrial thickness. The mean ± SD age of the cohort was 40.5 ± 6.6 years, gravidity was 1.8 ± 2.1 (range 0-7) and parity was 0.4 ± 1.1 (range 0-4); 76.2% of women had, based on age-specific FSH and anti-Müllerian hormone, an objective diagnosis of diminished ovarian reserve and had failed 2.0 ± 2.1 prior IVF cycles elsewhere.
MAIN RESULTS AND THE ROLE OF CHANCE:
With 5.2 ± 1.9 days between G-CSF perfusions and embryo transfers, endometrial thickness increased from 6.4 ± 1.4 to 9.3 ± 2.1 mm (P < 0.001). The Δ in change was 2.9 ± 2.0 mm, and did not vary between conception and non-conception cycles. A 19.1% ongoing clinical pregnancy rate was observed, excluding one ectopic pregnancy.
LIMITATIONS AND REASONS FOR CAUTION:
Small sample size (but a highly selected patient population) in an uncontrolled cohort study and in unselected first IVF cycles at our center.
WIDER IMPLICATIONS OF THE FINDINGS:
This pilot study supports the utility of G-CSF in the treatment of chronically thin endometrium and suggests that such treatment will, in very adversely affected patients, result in low but very reasonable clinical pregnancy rates.
STUDY FUNDING/COMPETING INTEREST(S):
This work was supported by the Foundation for Reproductive Medicine, New York, New York, USA, a not-for-profit research foundation and intramural grants from the Center for Human Reproduction (CHR)-New York. N.G. and D.H.B. are members of the board of the Foundation for Reproductive Medicine. N.G. is owner of CHR-New York, where the study was conducted. N.G. and D.H.B. have been recipients of research awards, travel grants and speaker honoraria from various pharmaceutical and medical device companies. None of these companies was, however, in any way associated with the materials and the manuscript presented here. N.G. and D.H.B. are listed as co-inventors on a number of awarded and still pending U.S. patents, none related to the materials presented here. N.G. is on the board of a medically related company, not in any way associated with the data presented here.
G-CSF treatment improves inadequate endometrium during IVF cycles
24. February 2011 03:26
During in vitro fertilization (IVF) cycles, treatment with a medication calledgranulocyte-colony stimulating factor (G-CSF) significantly improves inadequate endometrium (lining of theuterus), according to a report published electronically on February 15 in Fertility and Sterility - the official journal of the American Society for Reproductive Medicine (ASRM). The reported case series also suggests that G-CSF treatment may, in general, improve IVF pregnancy chances.
G-CSF is a cytokine (protein molecules that facilitate communication between cells) that has already been FDA approved for other clinical indications.
Researchers from New York City-based Center for Human Reproduction (CHR) and a second NY fertility center reported on four women with highly inadequate endometrium, unresponsive to conventional treatments and facing IVF cycle cancellation. In all four cases, endometrial perfusion of G-CSF expanded the endometrium to a minimal thickness of 7mm within approximately 48 hours, allowing for embryo transfer. Surprisingly, all four patients also conceived.
In approximately 1% of all IVF cycles, the endometrium stays too thin for embryos to successfully implant, even with treatment. In such IVF cycles, patients and physicians face two poor options: they either accept lower pregnancy chances and transfer embryos despite inadequate endometrium, or they can cancel the embryo transfer and freeze all embryos in hope of better future cycles. Unfortunately, women with inadequate endometrium often show inadequate endometrium again in future cycles. This situation was demonstrated by two patients in this reported case series with histories of repeat IVF failures due to thin endometrium.
"Conventional treatments for inadequate endometrium have had spotty success at best. Without G-CSF perfusion, these patients, likely, would not have reached embryo transfer," explains David Barad, MD, Director of Clinical ART at CHR and one of the senior authors of the report. "That all of them also conceived was a big surprise, and is, of course, quite remarkable."
"The efficacy of G-CSF in improving endometrium, and possibly pregnancy rates in general, still needs to be confirmed in randomized controlled trials," adds Norbert Gleicher, MD, lead author of the report and Medical Director of CHR. "Indeed, we already started two such trials to test both hypotheses; but until first results become available later in 2011, we caution against over-interpreting results of this small pilot study."
SOURCE Center for Human Reproduction

Fax: 04-7225626
e-mail: ok7260678@gmail.com
博元婦產科Twitter: http://twitter.
博元婦產科官方flickr http://www.




